Computer Vision Applications in Healthcare
By Dr. Sarah Kim
The fluorescent hum of a radiology reading room at 3:00 AM is a sound of quiet desperation. A single radiologist sits before a wall of monitors, eyes darting across the thousandth gray-scale image of the shift. Fatigue isn't just a personal grievance here; it is a clinical risk. When the human eye tires, the subtle shadow of a nodule or the faint hair-line fracture begins to blend into the noise of the anatomy. This is the bottleneck of modern medicine: we have become too good at capturing data and not yet fast enough at interpreting it. We are drowning in pixels, and for the first time, we are looking toward a non-biological lifeline to help us make sense of the deluge.
The Infrastructure of the Invisible
The meteoric rise of computer vision in medicine isn't just another tech trend; it's a structural necessity. By the end of 2023, the medical imaging AI market hit a valuation of $1.2 billion, but that number is a mere placeholder for the $10 billion explosion projected by 2030. This growth is fueled by a simple, brutal math: the volume of imaging data is increasing by nearly 5% annually, while the supply of radiologists is struggling to keep pace. We don't just need more doctors; we need doctors with bionic vision.
Regulatory bodies have finally shifted from skepticism to cautious embrace. The FDA has now cleared over 500 AI-enabled medical devices. The vast majority of these live within the realm of radiology, marking a paradigm shift in how we define a "medical device." We are moving away from scalpels and towards "Software as a Medical Device" (SaMD), where an algorithm's ability to detect a stroke is treated with the same clinical rigor as a physical heart valve.
Radiology's Second Set of Eyes
In the traditional workflow, a radiologist looks at a stack of images and dictates a report. In the AI-augmented workflow, the algorithm acts as a triage nurse, a proofreader, and a magnifying glass all at once. When a CT scan is performed on a patient suspected of having a stroke, every second counts. AI models now scan these images in the background, flagging large vessel occlusions (LVOs) and alerting the neurosurgical team before the radiologist has even opened the file. This isn't about replacing the doctor; it's about shifting the doctor's attention to where it is needed most urgently.
Chest X-rays remain the most common diagnostic tool in the world, yet they are notoriously difficult to read with 100% consistency. Recent work by Google Health has shown that deep learning models can identify pneumonia and tuberculosis with a sensitivity that rivals—and sometimes exceeds—board-certified specialists. This is particularly transformative in resource-strapped regions where a specialist might be hundreds of miles away. A laptop with a decent GPU becomes a world-class diagnostic hub.
MRI analysis is perhaps where the "vision" in computer vision becomes most impressive. Tools like nnU-Net have revolutionized medical image segmentation. Segmenting a brain tumor—manually tracing its boundaries across dozens of 3D "slices"—is a grueling task for a human. An AI can do it in seconds, providing precise volumetric data that allows oncologists to track whether a tumor is shrinking under chemotherapy with a level of accuracy the human eye simply cannot quantify.
The Cellular Needle in the Haystack
If radiology is about shadows, pathology is about textures. A single digital pathology slide can be several gigabytes in size, containing millions of cells. For a pathologist to find a cluster of ten metastatic cancer cells is like finding a specific grain of sand on a beach. This is where computer vision moves from "helpful" to "superhuman."
Companies like PathAI are training models to recognize the morphological signatures of cancer that are invisible to the naked eye. These systems don't just say "this is cancer"; they quantify the "spatial arrangement" of cells—how they interact with the surrounding immune system. This information is becoming vital for immunotherapy, where the physical location of T-cells relative to the tumor can predict whether a million-dollar drug will actually work. By digitizing the slide, we turn biology into a searchable, computable database.
Ophthalmology and the Window to the Soul
The eye is the only place in the body where we can see blood vessels and nerve tissue directly without cutting someone open. This makes it a goldmine for computer vision. The IDx-DR system became a landmark in medical history as the first FDA-cleared AI to provide a screening decision without the need for a clinician to interpret the image. It screens patients for diabetic retinopathy—the leading cause of blindness in working-age adults—in a primary care setting. This effectively moves the diagnosis from the specialist office to the local clinic, preventing vision loss before it begins.
Human vs. Machine: A Clinical Comparison
It is a mistake to view AI as a "better" version of a human. Instead, we should view them as having different, complementary skill sets. A human doctor understands context—the patient's family history, the look of fear in their eyes, the subtle "gut feeling" that comes from twenty years of practice. The AI understands statistics and pixel-level gradients. The following table breaks down this cognitive division of labor:
| Feature | Human Radiologist/Pathologist | Computer Vision System |
|---|---|---|
| Consistency | Variable (fatigue, mood, lighting) | 100% (identical results every time) |
| Contextual Knowledge | High (understands patient history) | Low (looks only at pixels) |
| Speed | Minutes to hours | Milliseconds to seconds |
| Pattern Detection | Excellent for known patterns | Superior for subtle, non-linear features |
| Handling Ambiguity | Strong (uses intuition) | Weak (requires confidence thresholds) |
The Technical Blueprint
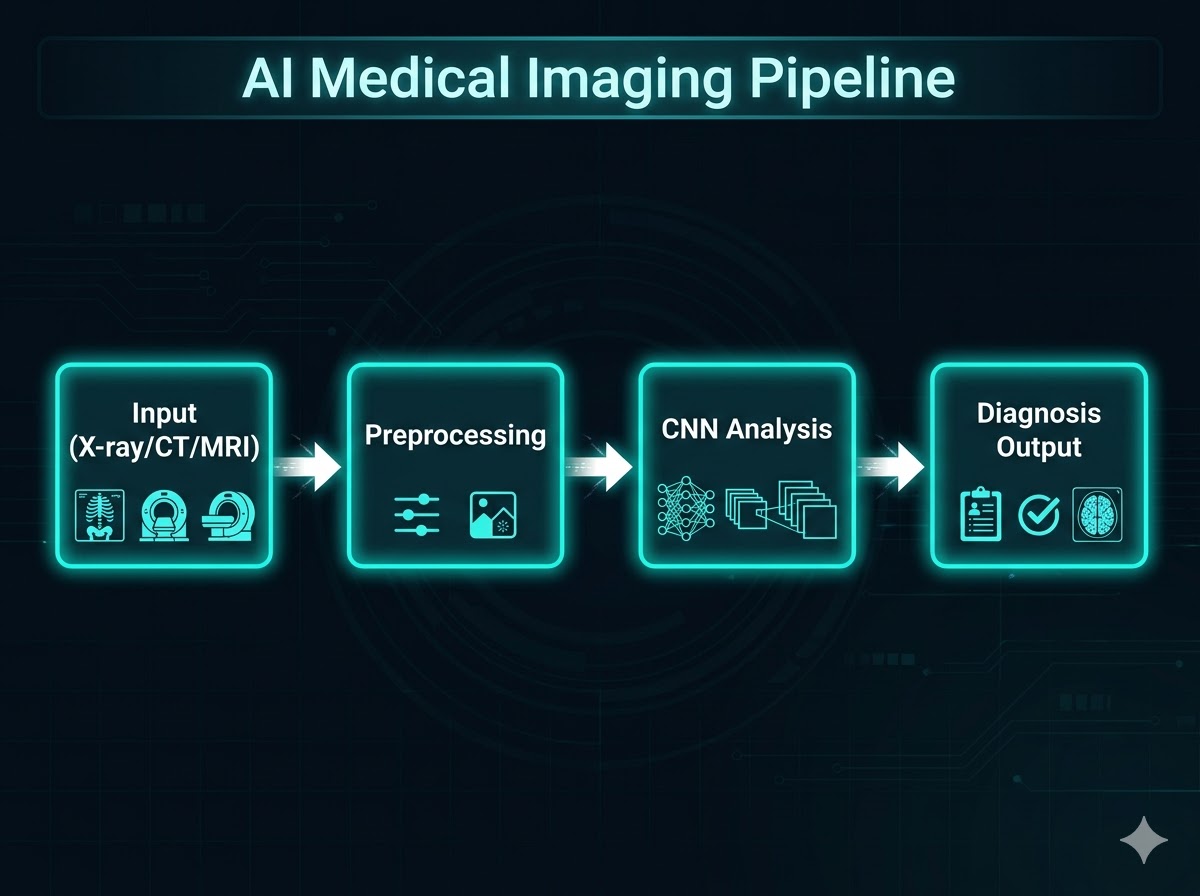
At its core, medical computer vision relies on Convolutional Neural Networks (CNNs). Unlike general-purpose AI, medical AI must be "radiology-aware." For developers and clinicians looking to implement these systems, the challenge isn't just the model; it's the pipeline. You cannot simply feed a raw DICOM file into a standard neural network and expect a diagnosis. You need a rigorous preprocessing and validation framework.
A Checklist for Clinical Deployment
- Data Diversity: Ensure training sets include images from different hardware manufacturers (GE vs. Siemens vs. Philips).
- Class Imbalance: In medicine, "normal" cases vastly outnumber "abnormal" ones. Use weighted loss functions to ensure the model doesn't ignore the rare, life-threatening pathologies.
- Explainability (Heatmaps): Never deploy a "black box." Use Grad-CAM or similar techniques to highlight why a model flagged a specific area.
- Integration: The model must live inside the PACS (Picture Archiving and Communication System), not on a separate website. If it adds three clicks to a doctor's day, they won't use it.
For those looking at the code, a basic preprocessing step often looks like this Python snippet using the pydicom and OpenCV libraries to normalize intensities:
import pydicom
import cv2
import numpy as np
def preprocess_medical_image(dicom_path):
ds = pydicom.dcmread(dicom_path)
image = ds.pixel_array.astype(float)
rescaled_image = image * ds.RescaleSlope + ds.RescaleIntercept
window_center = 40
window_width = 400
img_min = window_center - window_width // 2
img_max = window_center + window_width // 2
image_final = np.clip(rescaled_image, img_min, img_max)
image_final = ((image_final - img_min) / (img_max - img_min) * 255).astype(np.uint8)
return image_final
The Ghost in the Machine: Challenges and Ethics
Despite the optimism, we are currently navigating a "trough of disillusionment" regarding AI ethics. One of the most significant hurdles is algorithmic bias. If a model is trained primarily on data from Caucasian patients in urban academic centers, its accuracy may plummet when applied to patients of color or those in rural settings. In medicine, bias isn't just an issue—it's a patient safety hazard.
Then there is the "Black Box" problem. If an AI misses a tumor, who is responsible? The hospital? The developer? The radiologist who trusted the software? We are seeing a move toward "Augmented Intelligence" rather than "Artificial Intelligence," where the AI acts as a suggestion engine rather than a final authority. The goal is to keep the human in the loop, using the AI to filter out the noise so the human can focus on the signal.
We are also seeing the emergence of "Federated Learning," a technique where models are trained across multiple hospitals without the sensitive patient data ever leaving the hospital's firewall. This allows us to build powerful, diverse models while respecting the absolute sanctity of patient privacy.
The Road Ahead
The next frontier is multimodal AI—systems that don't just look at an image, but also read the patient's electronic health record, their genomic profile, and their wearable device data. Imagine a computer vision system that sees a faint shadow on a lung scan and cross-references it with a patient's recent cough and a genetic predisposition to small-cell carcinoma. We are moving from reactive "image reading" to proactive "health forecasting."
The fluorescent lights of the radiology suite will still hum at 3:00 AM. But in the near future, that exhausted doctor will have a digital partner that never sleeps, never blinks, and never gets bored. The pixels haven't changed, but our ability to see the life-saving truth hidden within them finally has.
References
- Moor, M., et al. (2023). "Foundation models for generalist medical artificial intelligence." Nature. https://www.nature.com/articles/s41586-023-05881-4
- Isensee, F., et al. (2021). "nnU-Net: a self-configuring method for deep learning-based biomedical image segmentation." Nature Methods. https://www.nature.com/articles/s41592-020-01008-z
- FDA. "Artificial Intelligence and Machine Learning (AI/ML)-Enabled Medical Devices." FDA.gov
- Abràmoff, M. D., et al. (2018). "Pivotal trial of an autonomous AI system for automated detection of diabetic retinopathy." Nature Digital Medicine.